

I’m sad to report that the manipulation of charitable patient assistance programs continues to expand. As you will see below, employers have significantly ramped up their adoption of AFPs, while health plans seem more skeptical. Meanwhile, a new AbbVie lawsuit sheds light on the alleged activities of a major AFP vendor.
Read on for our update on these suspect programs—and the growing risks to their sustainability. Caveat payer.
PAPs & AFPs
Here’s a brief refresher on how alternative funding programs (AFPs) operate.
Patient assistance programs (PAP) focus on patients who meet financial eligibility criteria—those without insurance and those denied coverage by their commercial plans. PAPs therefore differ from copayment offset programs that cover a commercially insured beneficiary’s out-of-pocket costs. Copayment offset programs may not be used by beneficiaries of any federal healthcare program, including Medicare Part D. PAPs can, however, support patients with government-sponsored insurance.
PAPs are often incorporated as 501(c)(3) nonprofit charitable foundations. Exhibit 134 of our 2023 Economic Report on U.S. Pharmacies and Pharmacy Benefit Managers lists 10 of the largest PAPs funded by pharmaceutical manufacturers.
PAPs enable alternative funding programs (AFPs), which are sometimes called specialty carve-outs. Here’s how the scheme works:
- Some or all specialty drugs are excluded from the plan’s formulary, so that a patient technically has no coverage (wink, wink) for the specialty drug.
- The excluded specialty drugs are then administered by secretive, private companies operating separately from the commercial plan’s PBM. Examples of these vendors include ImpaxRX, Paydhealth, PayerMatrix, SHARx, and Script Sourcing. (I won't promote these companies by linking to their uninformative web sites. Only two of the websites even bother to disclose the identity of the companies’ executives.)
- The vendor helps the patient disguise themselves as “uninsured” so they can apply for the manufacturer’s PAP funds to cover the cost of the prescriptions. (When contacting the manufacturer, some vendors will even impersonate the patient.) These prescriptions are typically filled by noncommercial pharmacies that are operated by specialty hub service companies funded by the manufacturer.
- The manufacturer ends up paying the full cost of the prescription and the pharmacy services. Meanwhile, the plan sponsor incurs no direct costs for the specialty drug.
- The plan pays the third-party AFP vendor a fee of up to 30% of the value of charitable funds provided to the patient, i.e., the drug's full list price. The vendor frames this excessive payout as a “cost avoidance” fee. Note that the fee is paid by the plan, not from the foundation's funds.
Employers and their highly-profitable vendors justify the use of charity funds in benefit plans by arguing that drug prices are “too high.” Therefore, the ends (free drugs) justify the means (bending or breaking the rules to loot a charity). You will surely not be surprised to learn that these vendors’ webpages never really explain how drug savings are generated—or how the vendors earn their profits.
As a comment on one of my Linkedin posts snarked: “There are many products and services in the US that I believe are too expensive for the value they bring. I steal none of them. I also don’t pay anyone else a commission to steal them on my behalf, nor do I pay any fees or commissions to a consultant who recommends different burgling services to me.” LOL!
LOOPHOLES R’ US
To evaluate the prevalence of AFPs, we rely on 2023 Trends in Specialty Benefit Design, the valuable new report from Pharmaceutical Strategies Group (PSG). (The report is free with registration.) For data on 2022 plan design, 104 employers and 45 health plans provided responses about their use of alternative funding programs. For data on 2021 plan design, we rely on the previous year’s survey, which included 114 employers and 30 health plans provided responses.
The results appear in the chart below. Due to the small sample sizes, I consider the results to be directionally correct, but they may not be representative of the whole population for either plan type.
Observations:
SUSTAINABLE?
As you can see above, a growing share of commercial payers are leveraging PAP loopholes to access need-based funds from charitable foundations that were established to help underinsured and uninsured patients.
In Section 6.2.3. of our 2023 pharmacy/PBM report, I highlight AFPs’ significant potential downsides for both plans and patients. These include reduced charity support, delayed treatment, higher administrative costs, vendor profiteering, and potentially serious ERISA- and IRS-related compliance issues.
And let’s not forget the ethical issues associated with misrepresenting the patient's financial situation and benefit coverage while also undermining the intent and operations of charitable patient assistance programs.
Consequently, controversy over AFPs is growing, as evidenced by these recent negative articles:
Going further, AbbVie sued Payer Matrix, one of the larger AFP vendors. Click here to read the complaint. AbbVie alleges multiple illegal activities associated with Payer Matrix's operations, including "Violations of Illinois Consumer Fraud and Deceptive Business Practices Act" and "Tortious Interference With Business Opportunity." Note that a complaint includes only the plaintiff's allegations, so Payer Matrix should be presumed innocent.
Even the plans that use AFPs are skeptical about the long-term viability of AFPs. Check out this fascinating chart from page 23 of PSG’s report:
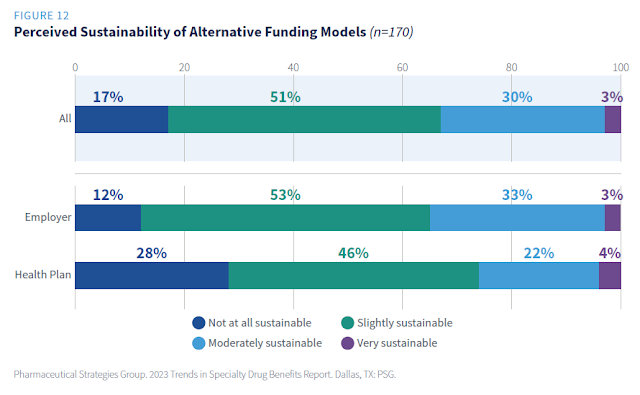
As you can see, a majority of employers and health plans believe that AFPs are either not at all or only slightly sustainable! Plans that currently use an AFP are somewhat more likely to view AFPs as sustainable. (This latter result came from an unreported cross-tab that PSG conducted at my request.)
Collective giving by the largest 10 pharmaceutical manufacturers’ PAP foundations was about $16 billion. With so much money sloshing around, we can expect AFP vendors to keep pitching their services, and plans to keep pretending they don’t know what’s really going on.
I expect AFP advocates to rely on the ultimate justification: The money doesn’t know where it comes from.
As a comment on one of my Linkedin posts snarked: “There are many products and services in the US that I believe are too expensive for the value they bring. I steal none of them. I also don’t pay anyone else a commission to steal them on my behalf, nor do I pay any fees or commissions to a consultant who recommends different burgling services to me.” LOL!
LOOPHOLES R’ US
To evaluate the prevalence of AFPs, we rely on 2023 Trends in Specialty Benefit Design, the valuable new report from Pharmaceutical Strategies Group (PSG). (The report is free with registration.) For data on 2022 plan design, 104 employers and 45 health plans provided responses about their use of alternative funding programs. For data on 2021 plan design, we rely on the previous year’s survey, which included 114 employers and 30 health plans provided responses.
The results appear in the chart below. Due to the small sample sizes, I consider the results to be directionally correct, but they may not be representative of the whole population for either plan type.
[Click to Enlarge]

Observations:
- Employers appear to be rapidly adopting AFPs. The share of employers currently using an AFP grew, from 6% of employers in 2021 to 14% in 2022. What’s more, employers with more than 10,000 covered lives were more likely to use an AFP. Per figure 38 of the PSG report (page 51), 17% of these employers reported currently using an AFP, compared with only 12% of smaller employers.
- Health plans seem to be more cautiously approaching AFPs. The reported share of health plans using AFPs dropped, from 10% in 2021 to 7% in 2022. The sample sizes are so small that this change is not really meaningful. However, I suspect that health plans are much more sensitive to the potential legal and regulatory risks of AFPs.
SUSTAINABLE?
As you can see above, a growing share of commercial payers are leveraging PAP loopholes to access need-based funds from charitable foundations that were established to help underinsured and uninsured patients.
In Section 6.2.3. of our 2023 pharmacy/PBM report, I highlight AFPs’ significant potential downsides for both plans and patients. These include reduced charity support, delayed treatment, higher administrative costs, vendor profiteering, and potentially serious ERISA- and IRS-related compliance issues.
And let’s not forget the ethical issues associated with misrepresenting the patient's financial situation and benefit coverage while also undermining the intent and operations of charitable patient assistance programs.
Consequently, controversy over AFPs is growing, as evidenced by these recent negative articles:
- Employers Use Patient Assistance Programs to Offset Their Own Costs, Kaiser Health News
- Patients Lose Access to Free Medicines Amid Spat Between Drugmakers, Health Plans, The Wall Street Journal
Going further, AbbVie sued Payer Matrix, one of the larger AFP vendors. Click here to read the complaint. AbbVie alleges multiple illegal activities associated with Payer Matrix's operations, including "Violations of Illinois Consumer Fraud and Deceptive Business Practices Act" and "Tortious Interference With Business Opportunity." Note that a complaint includes only the plaintiff's allegations, so Payer Matrix should be presumed innocent.
Even the plans that use AFPs are skeptical about the long-term viability of AFPs. Check out this fascinating chart from page 23 of PSG’s report:
[Click to Enlarge]

As you can see, a majority of employers and health plans believe that AFPs are either not at all or only slightly sustainable! Plans that currently use an AFP are somewhat more likely to view AFPs as sustainable. (This latter result came from an unreported cross-tab that PSG conducted at my request.)
Collective giving by the largest 10 pharmaceutical manufacturers’ PAP foundations was about $16 billion. With so much money sloshing around, we can expect AFP vendors to keep pitching their services, and plans to keep pretending they don’t know what’s really going on.
I expect AFP advocates to rely on the ultimate justification: The money doesn’t know where it comes from.
CORRECTION: An earlier version of this article incorrectly identified RxFree4me as a vendor that relies on PAP. While we classify RxFree4me as an alternative funding vendor, it relies partly on international sourcing rather than PAP.
No comments:
Post a Comment