

- Fresh evidence of 340B abuses by hospitals and contract pharmacies
- OptumRx rewrites its biosimilar Humira strategy
- ICER discovers channel markups
- Tax-exempt hospitals are not holding up their end of the bargain
P.S. Join my more than 41,000 LinkedIn followers for daily links to neat stuff. You can also find my daily posts at @DrugChannels on Twitter, where I have more than 16,400 followers. (I recommend that you follow me on LinkedIn, because the quality of comments is much higher than they are on Twitter.)
Speaking of PBMs, be sure to join me for my new live video webinar, PBMs and the Battle Over Patient Support Funds: Accumulators, Maximizers, and Alternative Funding, on June 23, 2023, from 12:00 p.m. to 1:30 p.m. ET. Click here to learn more and sign up.
340B Drug Discount Program: Information about Hospitals That Received an Eligibility Exception as a Result of COVID-19, United States Government Accountability Office
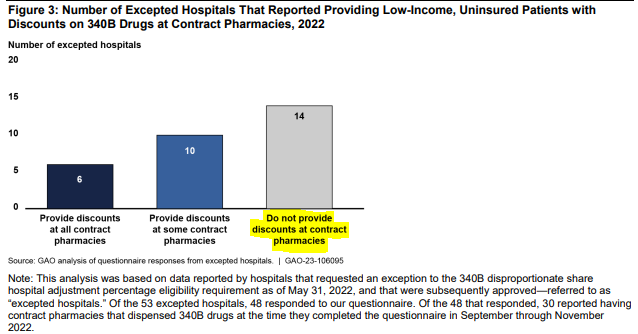
The Government Accountability Office (GAO) examined hospitals that requested a temporary exception to the 340B Drug Pricing Program’s eligibility requirements during the COVID-19 pandemic.
Unfortunately, the GAO uncovered evidence that again confirms our worst fears about how hospitals and pharmacies are abusing the 340B program. As you can see below from the report’s Figure 3, nearly half (14 out of 30) 340B hospital do *NOT* provide discounts to LOW-INCOME, UNINSURED patients at their facilities' contract pharmacies. Totally disgraceful!
Sadly, this is the THIRD government report to draw the same conclusion about hospitals’ inappropriate treatment of low-income, uninsured patients:
I don't believe a low-income, uninsured patient should ever pay full price for a deeply discounted drug simply to provide a hidden subsidy to a large, multi-billion-dollar health system and its for-profit PBM pharmacy partner. Apparently, many 340B advocates disagree with me on this point.
Unfortunately, the GAO uncovered evidence that again confirms our worst fears about how hospitals and pharmacies are abusing the 340B program. As you can see below from the report’s Figure 3, nearly half (14 out of 30) 340B hospital do *NOT* provide discounts to LOW-INCOME, UNINSURED patients at their facilities' contract pharmacies. Totally disgraceful!
[Click to Enlarge]

Sadly, this is the THIRD government report to draw the same conclusion about hospitals’ inappropriate treatment of low-income, uninsured patients:
- 2018: GAO Confirms It: 340B Hospitals and Contract Pharmacies Profit from Low-Income, Uninsured Patients.
I don't believe a low-income, uninsured patient should ever pay full price for a deeply discounted drug simply to provide a hidden subsidy to a large, multi-billion-dollar health system and its for-profit PBM pharmacy partner. Apparently, many 340B advocates disagree with me on this point.
Drug Channels News Roundup, April 2023, Drug Channels
It’s kind of cheating to link to a previous news roundup, but this development is simply too juicy to ignore.
As regular readers know, Amgen’s Amjevita, the first non-interchangeable biosimilar of Humira, launched with both a high-list/high-rebate and a low-list/low-rebate version of the drug. Reminder: List price = wholesale acquisition cost (WAC).
As I highlighted in last month’s roundup, one OptumRx formulary excluded the low WAC version—unless a plan chose to include it. (Lest you think I’m exaggerating, note that the formulary stated: “The low WAC products have been excluded…”) Another OptumRx formulary required patients to step through the high WAC version to get the low-WAC version, which presumably helped patients with...a clinical contraindication for a higher WAC?
These revelations were both embarrassing and ill-timed, given Congressional scrutiny on PBMs. So, shortly after I published my article, OptumRx’s PR team sprung into action. The formulary language was redrafted to make it harder to detect the default exclusion and step therapy requirements. See my original article so you can compare the original vs. revised language.
Here is OptumRx’s formal statement on this kerfuffle:
As regular readers know, Amgen’s Amjevita, the first non-interchangeable biosimilar of Humira, launched with both a high-list/high-rebate and a low-list/low-rebate version of the drug. Reminder: List price = wholesale acquisition cost (WAC).
As I highlighted in last month’s roundup, one OptumRx formulary excluded the low WAC version—unless a plan chose to include it. (Lest you think I’m exaggerating, note that the formulary stated: “The low WAC products have been excluded…”) Another OptumRx formulary required patients to step through the high WAC version to get the low-WAC version, which presumably helped patients with...a clinical contraindication for a higher WAC?
These revelations were both embarrassing and ill-timed, given Congressional scrutiny on PBMs. So, shortly after I published my article, OptumRx’s PR team sprung into action. The formulary language was redrafted to make it harder to detect the default exclusion and step therapy requirements. See my original article so you can compare the original vs. revised language.
Here is OptumRx’s formal statement on this kerfuffle:
“The low list NDC is not excluded and to ensure there is no confusion we clarified the language on our provider portal to reflect this. As we have shared previously, our clients have the choice to add or substitute the low list Amjevita NDC to either the Optum Rx Premium or Select formularies. The Premium Formulary simply defaults to the high WAC NDC based on client feedback and preference and can easily be configured to add in low WAC NDCs.”I’ll let you, dear reader, draw your own conclusions about OptumRx's apparent change of heart.
White Bagging, Brown Bagging, and Site of Service Policies: Best Practices in Addressing Provider Markup in the Commercial Insurance Market, Institute for Clinical and Economic Review (ICER)
Good news! ICER has finally discovered that channel markups "can be more than the price of the drug itself."
This insight was embedded within a decent report about the pros and cons of white bagging for provider-administered specialty drugs. I appreciated the inclusion of multiple reference to analyses published on Drug Channels, including our reviews of white-bagging, e.g., White Bagging Update 2022: Hospitals Battle to Boost Buy-and-Bill.
Over the years on Drug Channels, I have explained two primary reasons that a drug’s list price doesn’t reflect what a third-party payer actually spends for that drug: (1) channel intermediaries and providers add markups that account for the costs, profits, and value of their services, and (2) manufacturers provide rebates and discounts to drug channel particpants.
That’s why I found it so refreshing to see ICER take a break from bashing drug manufacturers to notice that hospitals inflate specialty drug costs by thousands of dollars per claim when compared with other channels. In many cases, hospitals earn thousands of dollars more than the drug’s manufacturer does.
Let’s hope ICER builds on its newfound insight.
This insight was embedded within a decent report about the pros and cons of white bagging for provider-administered specialty drugs. I appreciated the inclusion of multiple reference to analyses published on Drug Channels, including our reviews of white-bagging, e.g., White Bagging Update 2022: Hospitals Battle to Boost Buy-and-Bill.
Over the years on Drug Channels, I have explained two primary reasons that a drug’s list price doesn’t reflect what a third-party payer actually spends for that drug: (1) channel intermediaries and providers add markups that account for the costs, profits, and value of their services, and (2) manufacturers provide rebates and discounts to drug channel particpants.
That’s why I found it so refreshing to see ICER take a break from bashing drug manufacturers to notice that hospitals inflate specialty drug costs by thousands of dollars per claim when compared with other channels. In many cases, hospitals earn thousands of dollars more than the drug’s manufacturer does.
Let’s hope ICER builds on its newfound insight.
Testimony for the Record Submitted to the House Committee on Ways and Means Subcommittee on Oversight for the Hearing “Tax-Exempt Hospitals and the Community Benefit Standard”, Ge Bai, PhD, CPA
Speaking of 340B, I also recommend Ge Bai’s recent Congressional testimony. Dr. Bai argues that the 340B Drug Pricing Program is now a “buy-low-sell-high" tool for unaccountable hospital profits. She recommends some commonsense reforms, such as having hospitals report their gross profits from the 340B program.
Dr. Bai also offers potent critiques of tax exempt hospitals, noting:
Dr. Bai also offers potent critiques of tax exempt hospitals, noting:
“Many tax-exempt hospitals have adopted other revenue-enhancing activities that would normally be expected from for-profit entities, such as using anti-competitive tactics to retain market share and raise prices, failing to offer charity care to eligible patients, and employing aggressive debt collection practices.”The full testimony has numerous citations supporting her fact-based critiques of the out-of-control 340B program and hospitals’ behavior.
Choosing a Health Insurance Plan, Dr. Glaucomflecken
Dr. Glaucomflecken, the funniest physician on the internet, takes on the ever-growing complexity of U.S. health insurance. One of Dr. G.'s best videos yet, IMHO.
No comments:
Post a Comment